
Functional/Dilated Mitral Valve Disease
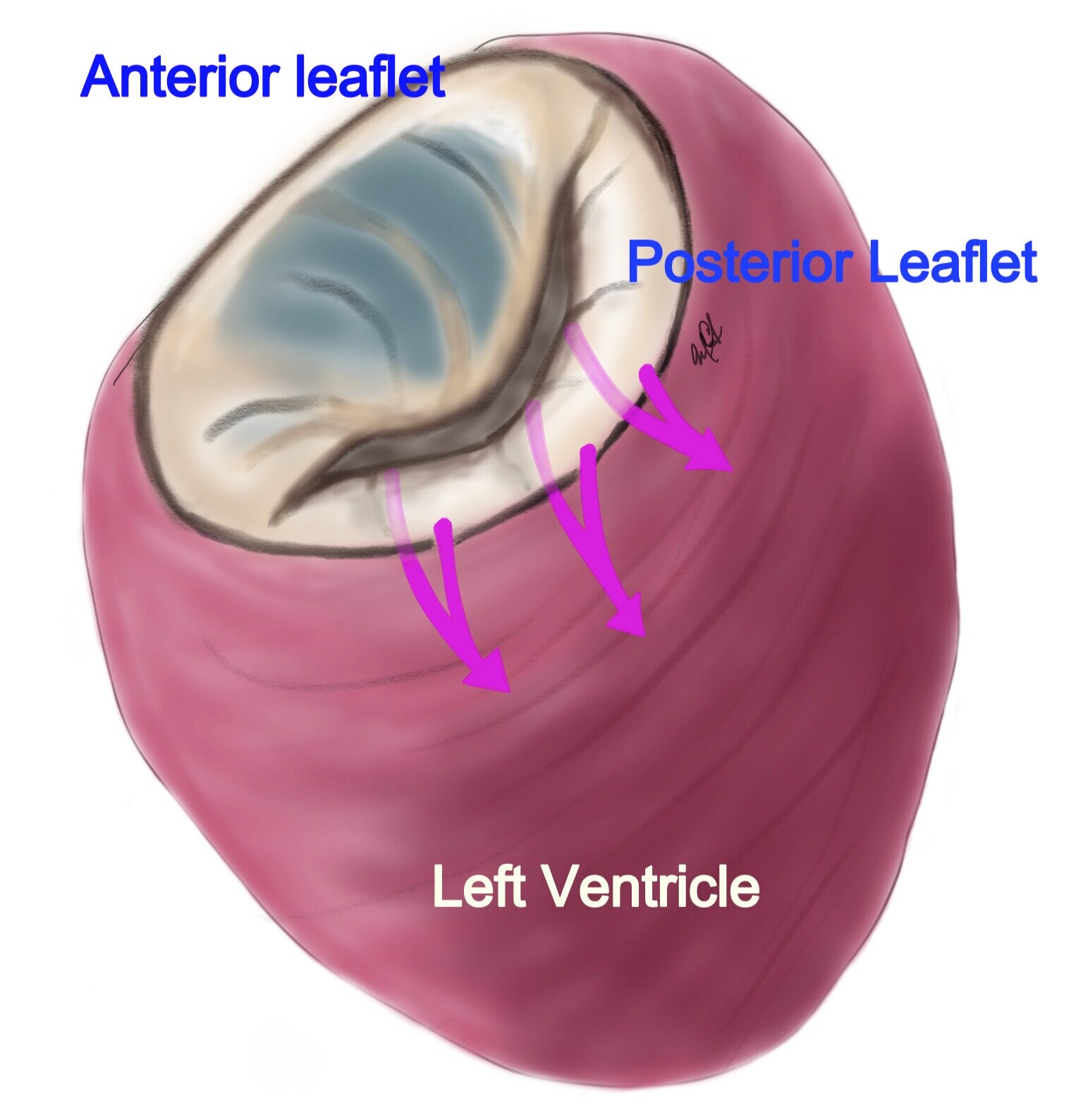
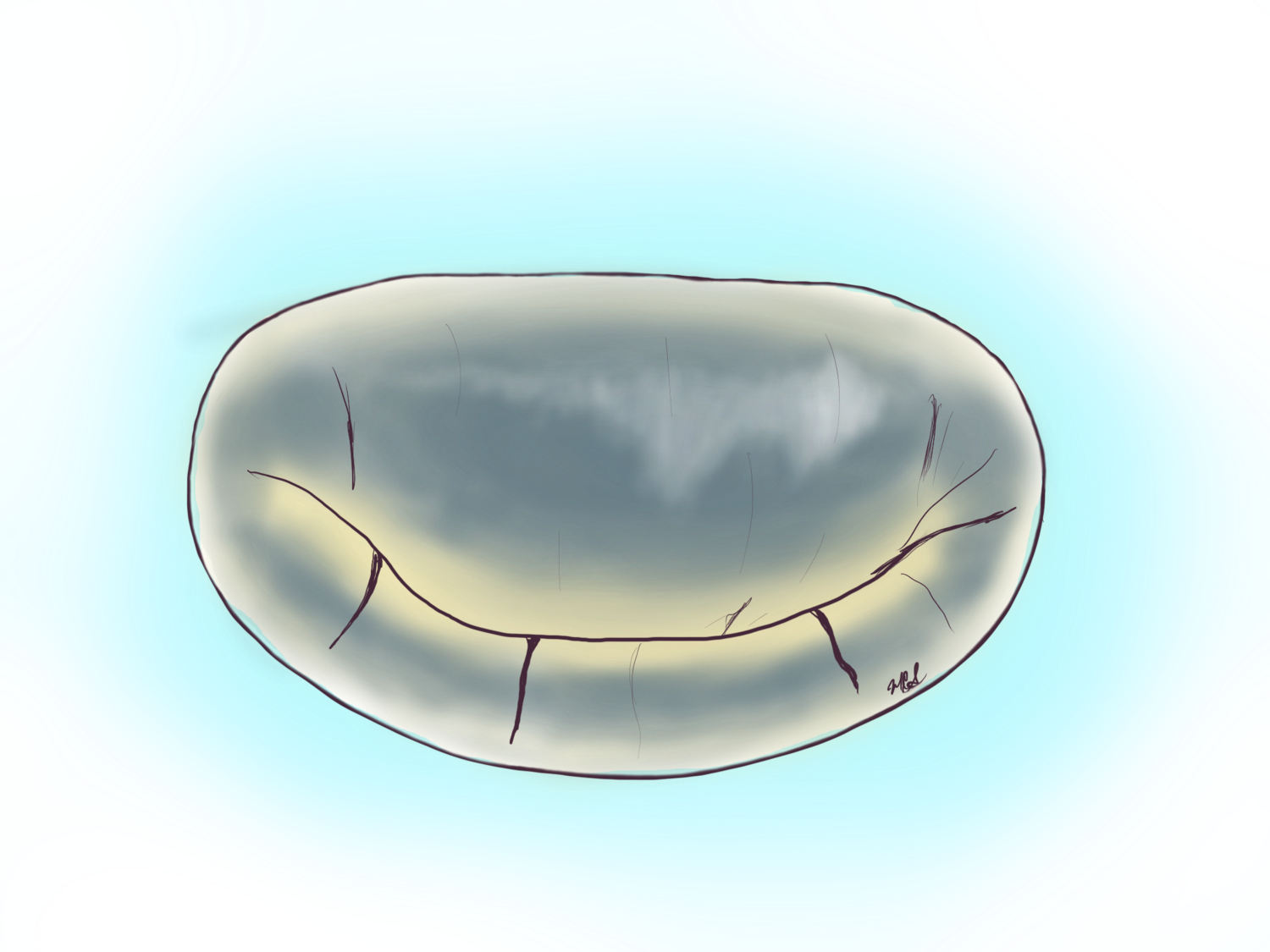
This image of the left ventricle and mitral valve shows the lower part of the heart with a more globular or balloon shape (rounded), this means it has enlarged or dilated and the annulus of the valve (black line around the mitral valve) has dilated and the two flaps of the valve are pulled apart.
Mitral regurgitation can take place in the absence of coronary blockages or ruptured chords. This typically takes place when the left ventricle undergoes dilation or enlargement and loses its conical shape remodeling to a more globular or spherical shape. Because it is not secondary to heart attacks it is called non-ischemic cardiomyopathy (or heart disease). This disease process is primarily a problem of the ventricular muscle and not the mitral valve proper.
The dilation, loss of contraction power and mitral leakage lead to further dilation which in turn splays out or pulls apart the two papillary muscles and these in turn pull on the chords and leaflets in opposite directions leading to the eventual loss of contact of the leaflets (loss of coaptation) and worse mitral leakage.
Take Home Points:
Ventricular dilation (non-ischemic cardiomyopathy) causes mitral leakage.
Functional mitral leakage is secondary to the dilation of the heart and its loss of power of contraction.
The best treatment for functional mitral regurgitation is evolving and warrants a discussion with a specialist.
The surgical repair of mitral regurgitation secondary to non-ischemic cardiomyopathy has not proven to be very successful as the loss of pump power of the ventricle is often irreversible at the time of presentation, but with medical management the symptoms of heart failure can be slowed down. Once severe mitral regurgitation takes place, when accompanied by profound loss of contraction power of the left ventricle, correcting the regurgitation does not recover the heart power, but may improve the symptoms of heart failure which include fatigue, weakness, shortness of breath, fluid overload with leg swelling or fluid accumulating around and in the lungs.
The management of this form of mitral regurgitation is still evolving with new therapies like the mitral clipping showing in one study to improve the symptoms as well as the life expectancy of these patients, while another study showed no improvement in life expectancy. In patients with profound loss of power (less than 30%) with severe mitral regurgitation one has to consider other therapies including left ventricular assist device implantation, heart transplantation as an open heart operation for mitral valve repair is unlikely to improve the power of the heart nor the longevity of the patient.

This trans esophageal echocardiogram shows the multiple leaking jets of mitral regurgitation. This leakage was brought on by the dilation of the annulus or “frame” that holds the two flaps of the valve. An analogy to a set of french doors is valid with the frame enlarging, but the leaflets or doors staying the same size.

This is a picture of the same valve seen on the picture to the left at the time of minimally invasive mitral valve surgery done with a 2 inch incision on the right chest.
THE DILATED (enlarged) HEART
In some people the left ventricle or left lower side of the heart dilates or enlarges for different reasons. This leads to the enlargement of the frame of the valve (dilated annulus) which leads to the lack of closure of the flaps and mitral leakage.